
The concept of Electronic Medical Records / Hospital Information Systems is on the rise, but it is very intriguing to understand when did doctors start to maintain patient records. Doctors did maintain medical records, but they were more for research and publishing papers. If you have seen old movies the doctor used to visit the patient at his/her home and give medications the doctor carries in his bag. I did not see the doctor write down anything or maintain any kind of record per say.

Documenting Medical Records came into the foray from 1920’s, obviously these were paper records. This is when patients were treated more in hospitals than at home of the patient. Managing the paper records was a big challenge and to help hospitals with the same there were Tabulating machines. One of the earliest machines used was the “Hollerith Tabulating Machine”.
Till this point there really wasn’t a standard methodology to document Patient Medical Records. Let us try and understand details of how the records were captured. Let us say a Patient ABC comes to the hospital complaining of stomach ache, the patient fills the forms waits for the Nurse to come. The Nurse comes and asks basic questions and documents the details asked on a Paper, these are called as Nurse Notes. After which the Doctor comes asks some more questions and documents the details – these are called as Physician notes.

The Doctor prescribes medications, Lab Test and an X-Ray. The Patient goes to the Lab gets the test’s done – at the end the patient gets the Lab Results. Similarly, the Radiologist would provide the X-Ray and results. All this data together will form the Medical Record, but there is a twist. From a Doctor’s point of view these are called as Source Oriented Medical Records. Any guesses why? Cause they are organized from the source where it was created
1. Nurse Notes
2. Physician Notes/Progress Notes
3. All Lab Results
4. All X-Ray Results
The data is good in terms of a Patient Medical Record, but it does not help track a problem which the patient has. Above all if a third person looks at the data he/she might not be able to interpret the problem with ease. In 1960’s Dr. Larry Weed came up with the concept of Problem Oriented Medical Records (POMR). Dr. Weed in his lectures mentions that some Doctors ask 5 questions and some 55, he emphasized that the questions should be based on Branching Logic and in 9 minutes one can gather lot of information related to the Patient. Overall, he mentioned that there are 4 phases of a POMR
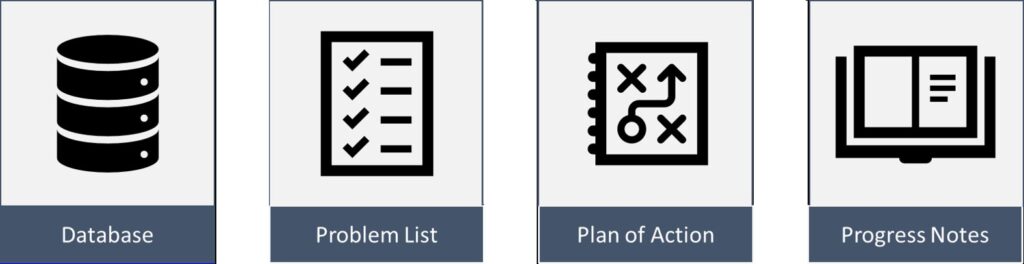
1. Maintain a Database – This has the Patients history, Physical and Lab Work etc.
2. A Problem List
3. Plan for each problem
4. Follow up Plan – Titled and Numbered Progress Notes.
Medical Records came into picture to help in maintaining Patient History, but another reason for their rise is they help in Audits, medical litigation (which saw and increase in 1960s) and for health insurance to decide rates and denials. As per practical experience of doctors, POMR was time consuming. After POMR, came the concept of SOAP notes which was an improved version of the same. In this case
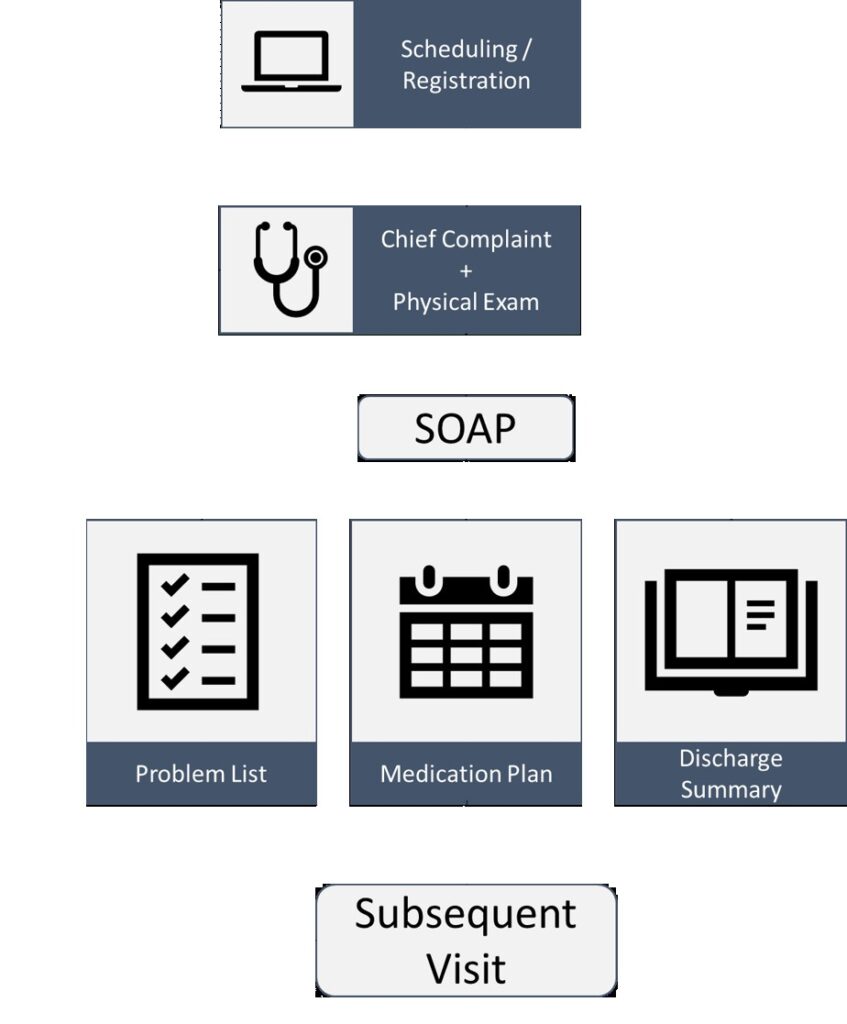
S, stands for Subjective which has details of the Patients Current Condition (Medical & Surgical History, Family & Social History).
O, stands for Observation/Objective which contains details of the Patient Vitals, Lab Tests and other observations.
A, stands for Assessment which is the Medical Diagnosis for that visit, and
P for Plan which is the Treatment Plan. This clinical documentation (in whatever format POMR or SOAP) helps the Medical Coders in entering the appropriate ICD code for billing purposes.

In 1970’s, Regenstreif Medical Record (RMR) one of the initial EMRs was developed by McDonald & associates and Indiana University School of Medicine. It was installed at Wishard Memorial Hospital in Indianapolis. The RMR was complimentary to the paper records not really replacing the same completely. By 1977, RMR was additionally storing Lab Results, X-Ray studies and ECG’s. The adoption rate of EMRs during this time was very low but still the billing and scheduling systems were being moved to computers. 1990’s saw the Advent of the Internet and EMRs were made available online and easy to access. The Institute of Medicine published Computer-Based Patient Record: An Essential Technology for Health Care, this was first of its kind document to explore possibilities of computerization of healthcare.

The document focused on different attributes (12 in total) such as Problem List, Clinical Reasoning, Data Entry, Clinical Problem Solving. The recommendation was for all Physicians to use Computers to improve Patient Care. 1996 saw a New law coming into picture in to deal with growing issues of Security and Privacy known as HIPAA. Feb 2009 brought a new law to not only implementing an EMR but also to Meaningfully use the EMR. This is where Hospitals are currently in 2018 trying to implement EMRs and meaningfully use them 🙂